December 1st, World AIDS Day (WAD), is a day to celebrate the lives needlessly lost to the HIV epidemic, to spread awareness of available HIV prevention and treatment, and to redouble our efforts to end the HIV epidemic globally.
This year, on WAD, I had the opportunity to speak with one of our local news stations here in NYC about the tools we have to end the HIV epidemic and how stigma remains a significant barrier.
In addition to stigma, racism, sexism, transphobia, and homophobia continue to contribute to stark inequities in HIV diagnoses.
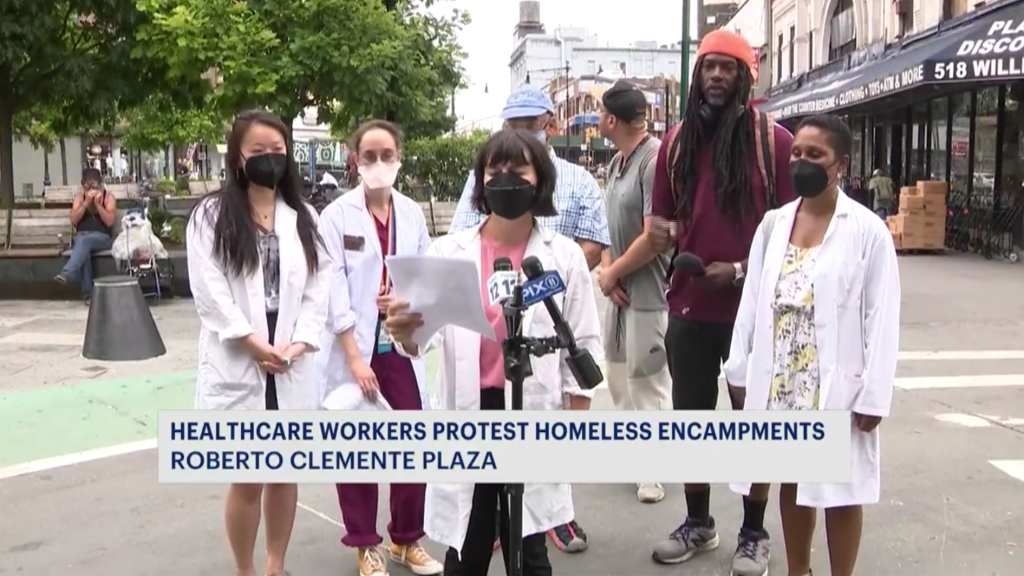
On July 25th, 2022, as a member of NY Docs, a coalition of diverse physician and healthcare advocates in the New York City area, Health Justice’s founder and ED, Dr. Oni Blackstock, shared remarks about the harms of street encampment sweeps to people impacted by homelessness and the need for safe and permanent supportive housing.
Below are Dr. Blackstock’s remarks that she delivered at the press conference hosted by NY Docs:
Good morning, Everyone!
I’m Dr. Oni Blackstock, founder and Executive Director of Health Justice, a racial and health equity consulting firm here in New York. I’m also a primary care and HIV physician and have had many patients who have experienced homelessness including living on the streets.
The administration says that its goal is to put NYers on a path to permanent housing and stability. They have couched this goal in a plan to improve “public safety”.
However, street encampment sweeps go a far way from that goal. Sweeps destabilize the lives of people on who are homeless harming their health and wellbeing of people. Sweeps are not leading to the stability or safe, accessible and permanent supportive housing that the administration claims to be its goal.
During sweeps, critically important medications are often thrown out—medications that people need to get through the day such as psychiatric medications and medication assisted treatment for opioid use disorder.
If people are unable to take meds for their chronic medical and psychiatric conditions, these conditions can worsen. For instance, loss of medication-assisted treatment can lead to withdrawal and increase substance use raising the risk for overdose or exposure to HIV and Hep C. Having one’s meds thrown out can increase in ED visits and hospitalizations.
Sweeps also make it harder for people who are homeless to connect with their health care providers because important items are destroyed during sweeps such as their phones and appointment reminder cards. Sweeps also make it more likely people will miss future appointments because they fear leaving their encampment sites because their items could be destroyed in yet another sweep.
Also, many people who are homeless are often disabled and require walkers, wheelchairs, and canes to get around—these have also been thrown out or destroyed during sweeps. It can be incredibly difficult for these items and medications to be replaced and can result in people being without their medications or assistive devices for weeks or even months.
The psychological stress of sweeps can be destabilizing. They increase stress, anxiety, and depressive symptoms. It’s inhumane to give someone 24 hours notice that the place they are living will be destroyed. Sweeps further compound the trauma that people who are homeless and living on the street have already faced. Involvement of the NYPD in sweeps ratchets up the risk of harm of the sweeps.
Sweeps can also be destabilizing to communities that people have created, networks of trust to support their health and wellbeing. Trust that allows people to leave their items and go to their medical appointments, that allow people to get help them if they overdose or if they need food.
They also shuffle people to new locations, which can be hazardous, isolated, less visible, places where people have less access to outreach workers and needed services.
The current status quo is clearly not working.
Many people who are homeless and living on the street have tried the shelter system especially congregate shelters. I know that from my experience talking to my patients, many have shared that they did not feel safe there and that their needs are not met- why send people back to somewhere where they feel unsafe and where their needs go unmet?
Congregate settings also ramp up the risk of getting COVID19 especially with BA.5—a hypertransmissable variant—and now we are dealing with the monkeypox public health emergency which could potentially spread easily in these settings.
Even if getting folks into shelters were a reasonable measure of success, these efforts are failing. Only a small proportion of people have actually taken the city up on its offer of housing in the shelter system. Many people remain unhoused and there are not currently enough safe haven and stabilization beds and few permanent housing options.
We are in the midst of housing and mental health crises.
The administration should be focused on permanent housing solutions and ensuring people experiencing homelessness get the health and social services that they need. We know that these both decrease homelessness and improve health outcomes for people who are homeless.
We need policies that support the health and safety of people who are homeless instead of policies that increase policing and criminalize poverty.
Health equity is about ensuring that all individuals and communities have access to the resources and opportunities that they need to attain optimal health and wellbeing. Key to creating and sustaining healthy communities is improving maternal health outcomes. I was honored to collaborate with Kelly Davis, Executive Director of New Voices for Reproductive Justice, and co-founder and CEO of Kinshift on this op-ed in response to U.S. Senator Bill Cassidy of Louisiana’s comments which placed the blame for his state’s high maternal mortality rate on Black birthing people themselves. We also address what needs to be done to ensure that Black birthing people have the supports needed to thrive and live their fullest lives. The op-ed can also be found here on New Voices for Reproductive Justice’s website.
The racialized health inequities revealed and amplified by the ongoing COVID pandemic, the continued threat to reproductive rights, and spiraling racist violence make recent comments by U.S. Senator Bill Cassidy of Louisiana about Black women and maternal mortality all the more appalling. During an interview discussing Louisiana’s maternal mortality rate – ranked among the highest in the country – the Senator remarked, “About a third of our population is African American; African Americans have a higher incidence of maternal mortality. So, if you correct our population for race, we’re not as much of an outlier as it’d otherwise appear.” He added, “Now, I say that not to minimize the issue but to focus the issue as to where it would be. For whatever reason, people of color have a higher incidence of maternal mortality.”
Since the remarks surfaced on the national stage, many people have expressed disbelief and outrage, even as Senator Cassidy refuses to retract his remarks. As Black health equity experts dedicated to addressing racism’s deleterious health impacts, we know that every part of Senator Cassidy’s analysis of Louisiana’s maternal mortality crisis contains glaring and willful obstructions of scientific facts and public health guidance. According to the Louisiana Health Department’s most recent data on pregnancy-associated mortality, Black birthing people accounted for nearly 60% of all maternal deaths in 2018 (despite representing 37% of births). However, Louisiana continues to fail all of its birthing people from this mostly preventable cause of death. White birthing people in Louisiana experience 53 maternal deaths per 100,000 births. In contrast, in New York the average white maternal mortality rate from 2016 to 2018 was 12.6. Simply put, the Senator’s assertion that to “correct [Louisiana’s] population for race” would align the state’s mortality rate is a lie.
The Senator’s remarks are just the newest insult to a festering moral injury that has plagued this nation since its inception. Rhetoric about “correcting” the population by presumably minimizing or disappearing Black people has been the baseline of centuries of eugenics and population control campaigns that have ascribed environmental degradation, poverty and poor health to the reproduction of people who are poor, disabled or non-white. These racist ideologies have not only informed decades of public policy and healthcare practice, but also undergird the current Replacement Theory national debate.
Systemic racism contributes to the feckless disregard for the sanctity of Black life in all sectors of society, including healthcare. Over 25 years ago, a group of Black women and femmes launched the Reproductive Justice movement which connects the need to name intersecting spheres of oppression and re-envision a world where Black women and gender-expansive persons can choose how and whether or not to have families, and thrive in safe and secure communities.
For Senator Cassidy to posit that there is no known root cause for the nation’s Black maternal health crisis flies in the face of global maternal health advocacy work that has been anchored by policy, advocacy and research catalyzed within his own state. The intense national news coverage about Black American maternal health has focused on Louisiana. National maternal, infant and reproductive thought leaders like the National Birth Equity Collaborative and Women With A Vision are helmed in New Orleans. A team of researchers led by Louisiana’s Tulane University proved that across the United State the risk for homicide actually increased during the perinatal period.
Senator Cassidy’s blaming Black people for poor health outcomes despite concrete evidence to the contrary is not happenstance, rather an age-old tactic used to evade the moral and political accountability of those in power. It’s easier for Senator Cassidy and others to shift the narrative to blame Black women than to use their power as leaders and legislators to create the social supports Black birthing people need to thrive like comprehensive health insurance, abortion access, gun control, and anti-racist medical care. Advancing even just one of these policy areas could drastically improve Louisiana’s maternal health. The ruling political class in Louisiana, including Senator Cassidy, has failed to meaningfully address any of these issues.
Irrespective of any politician’s contempt for the lives of Black birthing people, we know our liberation is not dependent upon the legislature. Black birthing people are the experts in what they need to thrive. By leading with equity and centering the needs of the most marginalized, politicians could help co-create pragmatic solutions to improve birth outcomes, not just in Louisiana, but across the globe. That should be Senator Cassidy’s ultimate goal. With or without him and other legislators, it will certainly be ours.
Kelly Davis is the Executive Director of New Voices for Reproductive Justice and the Co-Founder/Chief Equity Officer of KINSHIFT.
Oni Blackstock, MD, MHS is a primary care and HIV physician and founder and Executive Director of Health Justice.
It’s hard for me to believe that it’s been a full year since I officially launched Health Justice!
Admittedly, these times continue to be challenging for many of us as we head into the third year of the COVID-19 pandemic. The same social and health inequities that motivated me to found Health Justice remain or, worse, have been amplified. However, the energy from the social uprisings of 2020 and the collective desire for transformative change among many of us make the work of Health Justice more critical than ever. We’ve had a dynamic year of growth and learning supporting organizations in their respective equity journeys, and we eagerly look forward to more meaningful and generative engagements in our second year.
It’s World AIDS Day 2021—an opportunity to remember those who we have lost, the advances that have been made, and the work that still needs to be done to end the HIV epidemic.
Stark HIV-related inequities persist and Black and Latina men who have sex with men and Black and Latina cis and trans women in the U.S., continue to be disproportionately impacted by HIV. The COVID-19 pandemic has further complicated efforts to end the HIV epidemic. However, we have the tools we need to end both; we need the political will and resources to do so.
As tennis superstar and HIV advocate Arthur Ashe said during remarks on World AIDS Day in 1992
“We want to be able to look back and say to all concerned that we did what we had to do, when we had to do it, and with all the resources required.”
Dr. Oni Blackstock shares a few words about the meaning of World AIDS Day 2021 in the video below.
Global vaccine inequity continues to be a pressing concern with many countries, particularly those in sub-Saharan Africa, having severely limited access to COVID-19 vaccines. Dr. Blackstock, Health Justice’s founder and Executive Director, spoke on September 20, 2021, just steps from United Nations (U.N.) building in NYC where global leaders were convening for the U.N. General Assembly meeting, to speak out in support of global vaccine equity and to demand the US and other high-income countries support the Global South in developing the regional capacity to manufacture and disseminate COVID-19 vaccines. Below are Dr. Blackstock’s remarks:
Good afternoon!
Thank you to the organizers for the opportunity to speak with you today.
When I was young my parents would bring my twin sister and me to this very same spot to protest against racialized Apartheid in South Africa.
Today, I’m here to speak out against another form of apartheid—vaccine apartheid—which is also driven by the same systems of power, privilege and oppression as racialized apartheid.
As an HIV doctor and public health doctor—up until last year I was an Assistant Commissioner at the NYC Health Dept overseeing the city’s response to the HIV epidemic—I’ve had the opportunity to care for individuals, communities and an entire city—and this vantage point has shown me something that the pandemic has made abundantly clear—that our fates are inextricably linked. We saw that clearly as the Delta variant tore through India and ultimately became the cause of the 4th wave of the pandemic here in the US.
While boosters are being debated here in the US and other high-income countries, the World Health Organization reports that almost 6 billion vaccine doses have been administered globally, but 73% of all doses have been administered in just 10 countries. High-income countries have administered 61 times more doses per inhabitant than low-income countries.
This is important to me on many levels. My father was born in Jamaica and I have family who still live there. Just a stone’s throw away from the US and with a population of 3 million people, only about 200,000 people or 7% of the Jamaican population. Meanwhile, there are estimates that high income countries have procured around 1.5 billion excess doses.
Global vaccine inequity is a political choice. It does not have to be an inevitability.
These excess doses should be immediately donated to COVAX for urgent distribution to LICs and LMICs. We are already woefully behind in getting promised doses out. However, these charity donations are not enough. We need a sustainable way for countries in the Global South to make their own COVID-19 vaccines.
Vaccine manufacturing must be democratized.
In May of this year, President Biden put his support behind the TRIPS waiver which would waive intellectual property rights temporarily so that vaccine makers’ technology and know-how could be shared with other countries to manufacture life-saving vaccines. It would allow other producers to step in and make raw materials for export for all the current vaccines. It would also simplify agreements for eventual production of more doses.
As an HIV doctor, I want to emphasize that it is notable that the US put its support behind the TRIPS waiver. About two decades ago, when Brazil wanted to make its own generic versions of life-saving HIV medicines, the US government took legal action against Brazil, through the WTO, “claiming that Brazil’s production of generic HIV drugs breaks international laws on patent protection.” The US has frequently used threats of trade action against LICs and LMICs, to protect the US pharmaceutical industry.
So, Biden’s support for the waiver is an about-face from its previous stances. And the US is not alone in its support of the TRIPS waiver. The waiver is supported by over 150 countries. However, the largely influential European Union has not been supportive of the waiver.
For that reason, we call on President Biden to use the summit at the UN this week to persuade more countries especially those in the EU to support the TRIPS waiver and to cooperate with the US and other TRIPS waiver supporters in producing a draft of the WTO TRIPS waiver text.
But we know the TRIPS waiver alone will not solve COVID-19 vaccine inequity.
We urge President Biden to leverage the US government’s investments and legal authorities to transfer the technology from vaccine makers to support regional vaccine manufacturing in the Global South. For example, because its development was funded by us, US taxpayers, Biden could actually share Moderna’s recipe with the world. Moderna now has $12 billion in the bank. It’s time that Biden compel Moderna and other vaccine makers to share their technology more widely.
But, in order to manufacture more vaccines, we need LIC and LMIC need money.
We urge President to work with global leaders to identify and provide substantial funding for manufacturing vaccines in LICs and LMICs—funding that will support the building of new factories or retrofitting old ones and coordination of supply chains and other operational tasks at a global scale.
We will not be safe until everyone is safe.
Not ensuring global vaccine equity means more precious lives lost; it means prolonging the pandemic; it means potentially creating an even more dire situation with the emergence of more variants that could undermine existing vaccines’ efficacy.
Good afternoon, thank you to the organizers for inviting me to share a few words!
I’m Dr. Oni Blackstock—Founder of Health Justice, a health equity consulting firm; a member of New York Doctors, a coalition of health workers promoting health justice in NYC.
I’m also a primary care and HIV doctor. I did my medical training in the Bronx and spent much of my career practicing here.
In my role as a physician, I’ve come to understand very well the inextricable link between housing and health.
I’ve seen personally among my own patients how homelessness or having only temporary or unstable housing negatively impacts one’s ability to stay safe, to go to clinic visits and to take prescribed medications. And we know that the negative impacts of homelessness on health are only amplified during a pandemic.
And, yes, though the powers that be would have us believe otherwise, we are still in the midst of a pandemic.
COVID-19 is not behind us.
The city is still experiencing very high COVID-19 transmission.
We are now dealing with the more contagious Delta variant and, in the last two weeks alone, there has been a 138% increase in new COVID-19 cases.
Hospitalizations are starting increase again.
Now is not the time, nor is any time the time for that matter, but especially now, to be placing people who are homeless into congregate shelters.
We know that people experiencing street homelessness including those living in congregate shelters are older and have more chronic conditions and disabilities. In other words, they are at greater risk for severe outcomes due to COVID-19 such as hospitalization and death.
Transferring people from the safety of hotel rooms to congregate shelters in the middle of a pandemic is in effect a death sentence. It’s putting those who are among most vulnerable at THE greatest risk for getting COVID-19.
We know that housing is a prescription for good health and so to prevent a worsening crisis, we urge the Mayor to halt these unsafe transfers to congregate shelters immediately and to get individuals who are homeless into safe and stable housing.
We urge FEMA to continue to fund these hotel shelters during what continues to be the biggest public health emergency of the past century.
And, lastly, we call upon the Governor to sign the state bill that would increase housing vouchers to a fair market rate and this enable people to find permanent housing.
We must remember that none of us are safe until all of us are safe.
As efforts have intensified to get more Americans vaccinated, Health Justice is happy to share a healthcare provider training video that Health Justice developed with Advancing Health Equity for the NYC Health Department. The training video highlights how motivational interviewing techniques can be used to build patient confidence in and acceptance of COVID-19 vaccines.
Take a look and share with any health care providers who may find this content helpful!
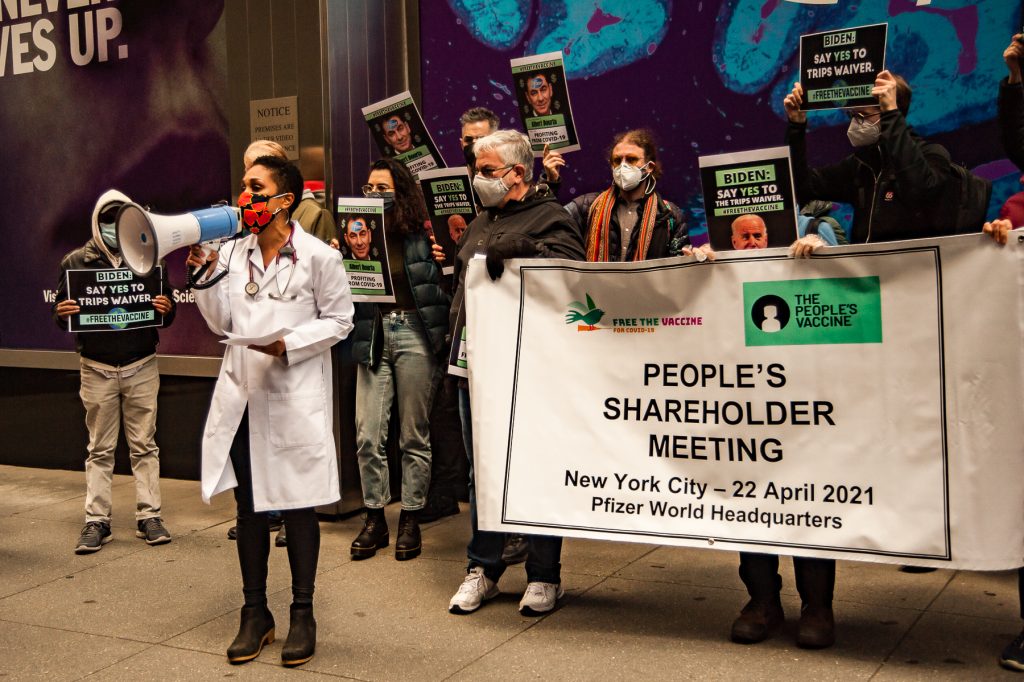
Dr. Oni Blackstock, Health Justice’s founder and Executive Director, recently participated in a protest outside Pfizer’s NYC headquarters to bring attention to and increase support for the critically important issue of global COVID-19 vaccine equity. Below she shares her remarks from this important protest:
I’m primary care and HIV doctor. I’m also a public health doctor—up until last year I oversaw NYC’s response to the HIV epidemic as an Assistant Commissioner at the NYC Health Dept.
These roles have allowed me to care for individuals, communities and an entire city—and this vantage point has shown me—what the pandemic has made abundantly clear—and that is that we truly are interconnected.
Yet, despite our undeniable connection to one another, all members of our society do not have equitable access to high quality healthcare or life-saving public health interventions. When this pandemic began, we immediately saw Black and brown communities disproportionately affected. And when it came to accessing the COVID-19 vaccine, the story was no different. This was due in large part to a lack of political will to ensure that the communities most burdened had equitable access to the vaccine.
And we’re seeing this same story play out globally.
Wealthy countries—countries that have created their wealth from the colonization and plunder of the most burdened countries—have hoarded vaccines instead of helping to ensure that less financially resourced countries have access to it.
My father was born in Jamaica and I have family who still live there. Just a stone’s throw from the US and with a population of 3 million people, Jamaica has only received 140,000 doses of vaccine. That’s it. That’s all the country has received. Meanwhile hundreds of millions of vaccines have gone to a dozen or so wealthy nations.
This is a political choice. Global vaccine inequity does not have to be an inevitability.
As an HIV doctor, I’m familiar with PEPFAR—the President’s Emergency Plan for AIDS Relief—it was an initiative that invested billions of dollars to make life-saving HIV treatment accessible to millions of people throughout the world. PEPFAR is a prime example of the ways in which the US government can contribute meaningfully and positively to global health if there is the will to do so.
While many of the US government policies have often either created or helped to sustain the socioeconomic conditions in the Global South, similar to PEPFAR, the US government now has the opportunity to start righting its wrongs and to do the morally correct thing to end this public health emergency.
We call on President Biden to use his powers to incentive vaccine makers such as Pfizer to share their know-how with other vaccine makers around the world especially in the Global South. We call on Pfizer and other vaccine makers themselves to share their vaccine-making knowledge. We also call on the President to support the TRIPS waiver which would allow generic and other producers in the Global South to manufacture life-saving COVID-19 vaccines.
The COVID19 pandemic will not be over here unless it’s over for everyone. Not ensuring global vaccine equity means more precious lives lost; it means prolonging the pandemic; it means potentially creating an even more dire situation with the emergence of more variants that could undermine existing vaccines’ efficacy.
This is the People’s vaccine.
We need global vaccine equity and we need it now. Thank you!
One aspect of starting Health Justice that has been very exciting was collaborating with graphic artist, Bryn Ludlow, to develop Health Justice’s logo. The logo colors were inspired by Jacob Lawrence’spaintings. Jacob Lawrence himself was inspired by the colors of Harlem, NYC. The figures are an H and J and the logo shows them coming together to nurture and grow Health Justice.
Take a look at this brief video to see the inspiration for the Health Justice’s logo and vision.
Justice at its best is love correcting everything that stands against love.
–Dr. Martin Luther King Jr.
2/1/2021
I’m thrilled to announce the launch of the website for Health Justice, my equity consulting practice, on this day, the first day of Black History Month 2021.
I created Health Justice to support health care, public health and other organizations in centering anti-racism and equity in their work with the vision of creating a world in which every human being and every community has the resources needed to achieve optimal health and well-being.
A desire to move our world towards one that is equitable and just was instilled in me by my parents. I vividly remember my mother and father taking my twin sister, Uché, and I to anti-apartheid and anti-racism demonstrations during our childhood and accompanying my mother, Dr. Dale Blackstock (also known as “the original Dr. Blackstock”) to community health fairs where she provided educational outreach. The latter experiences showed me how physicians can marry their clinical work with advocacy and service to advance equity.
My clinical, research and public health work in the HIV space has provided a lens through which to understand how systemic racism and other intersecting systems of oppression contribute to health and social inequities and has provided me with the opportunity to develop and implement programs and initiatives that work towards dismantling these systems which“sap the strength of the whole society through the waste of human resources”.
The current COVID-19 pandemic and last year’s social uprisings in support of Black Lives Matter have brought increased attention to the deleterious impact of systemic racism on health and has amplified existing inequities. If there were any moment to commit to transformational change, it is now. I’m excited for Health Justice to contribute to this moment and to creating a world in which everyone has the resources needed to thrive.